AI Speeds Cardiac MRI Breakthrough
AI Speeds Cardiac MRI Breakthrough
AI cardiac MRI is moving from flashy demo to clinical leverage, and that matters because heart imaging is one of medicine’s most valuable – and most bottlenecked – workflows. Cardiac MRI can reveal structure, scarring, blood flow, and function with remarkable detail, but it is also slow, expensive, and dependent on specialized experts who are already stretched thin. That mismatch has created a familiar problem across healthcare: powerful tools trapped behind operational friction. A new collaboration involving Carnegie Mellon University and Cleveland Clinic signals something more useful than hype. The real story is not that artificial intelligence can “see” the heart. It is that AI may finally help hospitals acquire, process, and interpret complex scans faster enough to change who gets access, when they get diagnosed, and how confidently clinicians can act on what they find.
- AI cardiac MRI targets one of healthcare’s biggest imaging bottlenecks: long, expert-heavy heart scans.
- CMU and Cleveland Clinic’s work points to AI that can improve image acquisition, reconstruction, and analysis.
- Faster workflows could mean broader access, lower operational strain, and earlier detection of serious heart disease.
- The biggest question is not whether AI can assist radiology – it is whether it can fit safely into real clinical practice.
Why AI cardiac MRI matters now
Cardiac MRI has long been considered a gold-standard imaging option for evaluating the heart. It can help clinicians assess cardiomyopathy, inflammation, ischemia, congenital abnormalities, and tissue damage with a level of precision that other modalities often cannot match. The problem is throughput. These exams can be lengthy, technically demanding, and vulnerable to motion artifacts caused by breathing or heartbeat variability.
That creates a brutal tradeoff. Hospitals want the diagnostic value of MRI, but they also need schedules that move, staffing models that work, and scans that do not have to be repeated because of poor image quality. This is where AI becomes strategically important. Not as a replacement for cardiologists or radiologists, but as a layer that can reduce friction across the entire imaging chain.
The most meaningful healthcare AI does not replace expertise. It compresses time, reduces error, and extends scarce specialist capacity.
That is why this collaboration deserves attention. The promise is not abstract intelligence. It is workflow intelligence.
Where the technology could make the biggest impact
When people hear about AI cardiac MRI, they often jump straight to diagnosis. But the most immediate benefits may appear earlier in the process.
1. Faster image acquisition
Traditional cardiac MRI requires multiple sequences and patient cooperation over a relatively long scan. AI-assisted acquisition can potentially reduce how much raw data must be collected while still preserving clinical quality through reconstruction methods. In practical terms, that could shorten scan times and make imaging easier for sicker patients, older adults, or anyone who struggles to remain still.
That matters operationally. A shorter exam is not just a better patient experience. It can also increase scanner availability, reduce backlog, and make high-end imaging more financially sustainable for health systems.
2. Better image reconstruction
One of the most promising uses of machine learning in MRI is turning limited or noisy input into diagnostically useful images. In cardiac imaging, where motion is a constant obstacle, better reconstruction can mean fewer unusable studies and less time spent rescanning.
If the CMU and Cleveland Clinic effort focuses on reconstruction pipelines, the upside is substantial. Better reconstructed images can improve downstream analysis and reduce the variability introduced by difficult acquisition conditions.
3. Automated segmentation and measurement
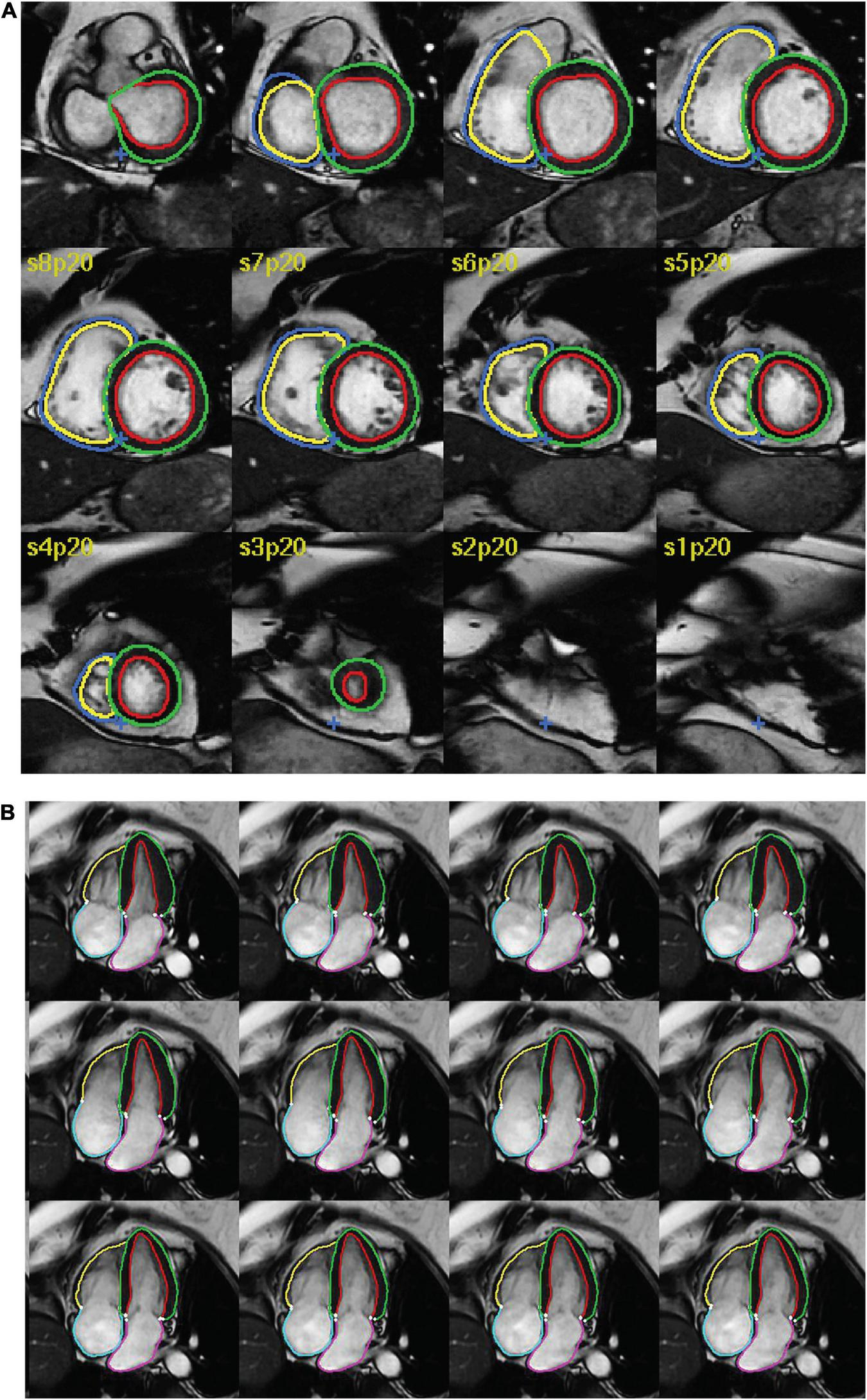
Cardiac MRI analysis often involves labor-intensive tasks such as outlining the heart chambers, measuring ventricular volumes, estimating ejection fraction, and identifying tissue abnormalities. AI models can automate parts of this work, potentially turning what once required lengthy manual review into a faster and more standardized process.
For clinicians, that could mean less time tracing anatomy and more time making decisions. For patients, it could mean results arrive sooner.
4. Risk stratification and decision support
The more ambitious layer is predictive insight. Once AI can reliably extract structured features from imaging, it can support models that flag patterns associated with heart failure, fibrosis, arrhythmia risk, or progression of disease. That does not mean algorithms should dictate care. It means they can surface signals clinicians might use to prioritize follow-up, tailor treatment, or spot subtle changes earlier.
The CMU and Cleveland Clinic angle is what makes this credible
Academic-medical collaborations often sound good in press materials, but this pairing has real logic behind it. Carnegie Mellon brings serious depth in artificial intelligence, computational modeling, and data science. Cleveland Clinic brings what many AI projects lack: access to real clinical workflows, domain expertise, and the operational reality of deploying advanced tools in patient care.
That combination matters because healthcare AI usually fails in one of two ways. Either the model is technically impressive but detached from bedside reality, or it is clinically relevant but too crude to scale. A partnership like this has a better shot at bridging both sides: algorithmic sophistication and practical utility.
It also signals a maturing phase for medical AI. The sector is moving beyond broad claims about “AI for healthcare” and toward narrower, higher-value applications where performance can be measured against specific outcomes: scan duration, image quality, reporting time, reproducibility, and diagnostic confidence.
The future winners in healthcare AI will not be the loudest platforms. They will be the tools that fit naturally into existing clinical systems and quietly save time without sacrificing trust.
Why hospitals should care about AI cardiac MRI
For health systems, this is not just a research story. It is a capacity story.
Demand for advanced imaging continues to rise while staffing constraints remain very real. Experienced cardiac imagers, MRI technologists, and subspecialty readers are not easy to hire, and burnout is a persistent issue. If AI can reduce manual steps, accelerate post-processing, and improve first-pass image quality, it can act as a force multiplier.
- Higher throughput: More patients scanned per day without compromising quality.
- Lower repeat rates: Better image capture and reconstruction can reduce wasted appointments.
- More consistent reporting: Automated measurements may help standardize interpretation.
- Improved access: Community sites may gain stronger support for advanced imaging programs.
This is especially important as cardiovascular disease remains a leading cause of death globally. Any technology that helps clinicians move faster on diagnosis without lowering the standard of care deserves serious scrutiny – and serious attention.
The skepticism is healthy and necessary
None of this should be accepted uncritically. Healthcare has already seen enough AI overpromising to justify a more skeptical lens.
Clinical validation is everything
An AI model that performs well on curated research data may fail in a busy hospital where patients move, devices vary, and protocols differ. Cardiac MRI is particularly sensitive to real-world complexity. Validation must cover diverse populations, scanner types, institutions, and disease categories.
Workflow integration is harder than model design
Even excellent models can create friction if they are bolted awkwardly onto clinical systems. If a radiologist has to open a separate tool, verify multiple outputs manually, or troubleshoot inconsistent behavior, adoption drops fast. The best implementations disappear into the workflow.
Explainability still matters
Clinicians do not need every neural network to be fully interpretable at the mathematical level, but they do need confidence in what a system is measuring, where it might fail, and how to verify its outputs. In medicine, opacity is not a feature.
Bias and access can cut both ways
AI may improve access to advanced imaging, but only if the models are trained and tested across varied patient groups. Otherwise, efficiency gains for some populations could coexist with degraded performance for others. That is not just a technical issue. It is a care quality issue.
What this could change for patients
If this work delivers on its promise, patients may notice benefits in practical, non-hyped ways.
They may spend less time in the scanner. They may get results faster. Their doctors may have more precise measurements and clearer visuals to guide treatment. In some cases, hospitals that previously struggled to operationalize advanced cardiac MRI at scale may be able to offer it more consistently.
That kind of impact often gets lost in AI coverage because it sounds incremental. It is not. In healthcare, incremental improvements in speed, reliability, and consistency can produce very large outcomes when applied across thousands of cases.
For someone with suspected cardiomyopathy or unexplained cardiac symptoms, a faster path from scan to diagnosis can reduce uncertainty and accelerate treatment decisions. That is where this technology stops being a systems story and becomes a human one.
Pro tips for evaluating any AI cardiac MRI platform
Healthcare leaders, radiology teams, and clinical buyers should ask sharper questions than vendors often invite.
- Ask what problem is actually being solved:
acquisition,reconstruction,segmentation,reporting, or all of the above. - Request real-world performance data: not just internal benchmarks.
- Look for workflow fit: Can the system integrate with existing
PACS, reporting tools, and MRI operations? - Verify clinician oversight: Human review should remain central, especially in edge cases.
- Measure outcome value: Track scan time, repeat rates, turnaround time, and diagnostic confidence.
Those questions separate useful clinical AI from software theater.
What comes next
The next phase for AI cardiac MRI is likely to be less about headline-grabbing novelty and more about disciplined deployment. Expect tighter focus on measurable improvements: reducing scan duration, automating repetitive analysis, and generating structured outputs that clinicians can trust.
Longer term, the bigger opportunity is multimodal care. Imaging data combined with EHR records, labs, genetics, and monitoring data could help build richer models for cardiovascular risk and treatment planning. But that future only works if today’s imaging AI proves it can be safe, reliable, and clinically useful on its own.
The CMU and Cleveland Clinic collaboration is compelling because it targets exactly the kind of problem AI should solve: a high-value medical workflow constrained by time, complexity, and expertise shortages. If the effort succeeds, it will not just make MRI smarter. It will make advanced heart imaging more available, more efficient, and more actionable.
That is the real breakthrough: not machines replacing doctors, but systems finally helping good clinicians move at the speed modern medicine demands.
The information provided in this article is for general informational purposes only. While we strive for accuracy, we make no guarantees about the completeness or reliability of the content. Always verify important information through official or multiple sources before making decisions.


