Gut Fermentation Disorder Demands New Clinical Playbook
Autobrewery syndrome has long lived at the fringes of medical conversation, dismissed as myth or excuse, yet it is rapidly becoming a flashing warning light for anyone who trusts their gut more than their lab results. Imagine waking up with the slurred speech and spinning room of a hangover after a sober night, or facing a surprise DUI because your intestines brewed their own ethanol. That is not speculative fiction; it is a metabolic glitch born from microbial overgrowth and sugar-heavy diets that modern healthcare often misses. The stakes are human liberty, road safety, and the credibility of clinicians who still lean on outdated heuristics. With hospital systems under pressure to triage faster and insurers scrutinizing every test, recognizing this condition early could mean the difference between treatment and legal fallout.
- Autobrewery syndrome can spike endogenous
blood alcohollevels without a drink. - Diagnostic blind spots persist because symptoms mimic intoxication and IBS.
- Dietary shifts, antifungals, and targeted probiotics can rebalance the
gut microbiome. - Courts are beginning to consider medical evidence when DUIs involve unexplained ethanol spikes.
- Future wearables and continuous sensors could track fermentation risk in real time.
Autobrewery Syndrome Basics
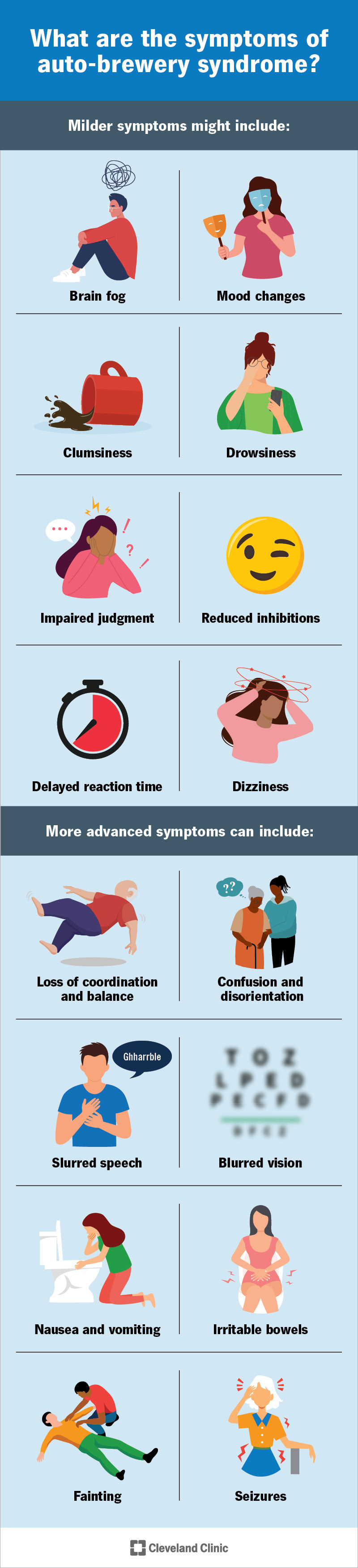
At its core, autobrewery syndrome is a metabolic derailment in which fungi or bacteria convert carbohydrates into ethanol before the liver can intervene. The phenomenon hinges on the interplay between the gut microbiome, mucosal immunity, and dietary load. When organisms like Saccharomyces cerevisiae or certain Klebsiella strains overgrow, they hijack the digestive tract, effectively turning the small intestine into a brewery. Patients report dizziness, cognitive fog, and the same slurred speech that officers equate with intoxication, yet their drinking history is nonexistent. This disconnect undermines trust between patients and providers who are conditioned to assume behavioral causes before biological ones. Understanding the mechanism reframes the gut not as a passive tube but as a metabolic reactor whose byproducts can alter legal status and cognitive function in minutes.
What Happens Inside the Gut
The intestinal lumen becomes a fermentation vat when excess simple sugars saturate the diet and antifungal surveillance falters. Yeasts feast on glucose, producing ethanol that is absorbed through the portal vein and floods the bloodstream. Unlike socially consumed alcohol, endogenous ethanol lacks the sensory cues that alert the drinker, so individuals may attempt to drive or work unaware of their rising blood alcohol levels. The liver, already tasked with detoxifying environmental pollutants, cannot clear the surprise surge quickly enough, creating transient spikes that mimic binge drinking. Nutrient imbalances, low gastric acid, and prior antibiotic courses set the stage for this takeover, illustrating how standard Western lifestyles can weaponize the microbiome against its host.
Why Diagnosis Lags
Clinicians default to more common explanations like covert drinking, drug interactions, or panic attacks. The rarity of documented cases keeps autobrewery syndrome off differential lists, while standard panels skip fermentation markers. Breath tests are typically deployed by law enforcement, not gastroenterology clinics, and even when ordered, timing matters: fasting or low-carb meals may yield normal results, masking intermittent episodes. Insurance protocols discourage exploratory testing, and many providers have limited access to gut fermentation assays or specific stool cultures. This diagnostic inertia prolongs patient stigma and delays the dietary and microbial interventions that could shut down the unwanted ethanol factory.
Autobrewery Syndrome Signals Clinicians Miss
The telltale pattern is cyclical fogginess after carb-heavy meals, escalating to coordination problems that subside without clear triggers. Family members may notice mood swings or sudden sleepiness. These signs are easily mislabeled as depression, hypoglycemia, or anxiety, especially when patients already manage irritable bowel symptoms. Primary care visits often focus on surface complaints, leaving the metabolic link untested. A willingness to ask whether breathalyzer readings ever appeared unexpectedly can be the diagnostic unlock.
Misattribution to Alcohol Use
Because ethanol is the endpoint, doctors and employers assume intent. That bias has legal consequences: DUIs, workplace suspensions, and child custody disputes can hinge on a lab report stripped of context. Patients are trapped in a feedback loop of disbelief, forcing them to prove sobriety while battling a microbiological problem. Breaking that loop demands clinician education and standardized protocols that treat unexplained ethanol as a red flag for further testing, not character judgment.
Testing Challenges
Confirming the condition requires a controlled carbohydrate challenge followed by serial blood alcohol and stool culture measurements. Many clinics lack the time or reimbursement to run these protocols. False negatives arise when patients unknowingly restrict carbs before testing or when fungal loads fluctuate. Portable continuous alcohol sensors, currently marketed for sobriety programs, could be repurposed to capture spikes correlated with meals, offering evidence between office visits. Laboratory capacity for sequencing and quantifying gut fungi remains uneven, slowing mainstream adoption.
Clinical Management Playbook
Once identified, management borrows from infectious disease, nutrition, and behavioral medicine. Antifungal agents such as fluconazole can reduce yeast burden, but they must be paired with diet restructuring to prevent relapse. High-protein, low-simple-carb plans deprive fermenters of fuel. Targeted probiotics and prebiotics aim to crowd out ethanol-producing strains, though evidence is still emerging. Patients also need strategies for acute episodes: if dizziness hits, self-testing with a personal breathalyzer can inform whether to avoid driving or operating machinery. Close collaboration with dietitians and pharmacists helps tailor interventions that minimize drug-nutrient interactions.
Diet as First-Line Defense
Carbohydrate periodization, where patients cluster complex carbs around times of high liver capacity and pair them with fiber, can blunt ethanol production. Eliminating refined sugars for several weeks often yields dramatic symptom reduction. Fermented foods that contain live cultures require caution; while they promote gut diversity, they may also feed opportunistic yeasts. Logging meals alongside subjective symptoms and any sensor readings builds a personal dataset that clinicians can act on, turning a mysterious condition into a trackable variable.
Medication and Monitoring
Antifungals carry liver load, so baseline hepatic panels and follow-up tests are crucial. Some cases respond to non-absorbed agents that act locally in the intestine, reducing systemic side effects. Betaine HCl or digestive enzymes are sometimes trialed to boost gastric defense. Wearable alcohol monitors or smart breath sensors provide behavioral feedback loops, alerting patients when their gut chemistry is drifting. Integrating these devices into electronic health records could automate alerts for clinicians when readings breach safe thresholds.
Legal and Ethical Fault Lines
Autobrewery syndrome is colliding with legal frameworks built on personal responsibility. Courts are beginning to weigh medical documentation as mitigating evidence, but standards are inconsistent. Defendants may need to demonstrate documented episodes, clinical diagnosis, and adherence to treatment plans. There is also a privacy dimension: continuous monitoring creates sensitive data that could be subpoenaed or misinterpreted. Employers who mandate alcohol testing must distinguish between substance misuse and metabolic anomalies, or risk wrongful termination claims.
Key insight: Treating unexplained intoxication as a medical signal rather than a moral failing aligns legal outcomes with biological reality.
Ethically, physicians must balance patient advocacy with public safety. Advising a patient to avoid driving during dietary transition periods is prudent, but so is providing them with tools and documentation to prove their condition if questioned by law enforcement. Clear communication reduces stigma and prevents adversarial encounters.
Why This Matters for Public Health
Autobrewery syndrome exposes gaps in metabolic literacy across healthcare systems. It underscores how the microbiome can swing from ally to adversary based on diet, medication history, and stress. The condition also highlights inequities: communities with limited access to fresh food or gastroenterology specialists may face higher risk and lower detection. Public health campaigns that frame gut health as integral to cognitive and legal wellness could shift dietary norms and testing protocols, reducing collisions, workplace incidents, and ER visits driven by mysterious intoxication.
Future Tech and Research
Continuous ethanol sensors, already shrinking in size, could become standard features in fitness wearables, alerting users to fermentation events alongside heart rate and glucose. Machine learning models trained on diet logs, stool sequencing, and sensor data might predict when a gut is primed to brew ethanol, enabling preemptive diet adjustments. Clinical trials that map which probiotic strains most effectively outcompete ethanol producers could turn this from a niche curiosity into a treatable metabolic syndrome. Insurance coverage will follow evidence, so rigorous, multi-center studies are the next strategic step.
Pro Tips for Clinicians and Patients
For clinicians: add unexplained intoxication to differential diagnoses, order carbohydrate challenge tests when history suggests cyclic symptoms, and document episodes to support patients in legal settings. For patients: carry a personal breathalyzer, track meals and symptoms in an app, and involve a dietitian early. Ask your provider about short-course antifungals and microbiome-friendly diets rather than relying on over-the-counter remedies that could worsen yeast overgrowth.
Actionable Playbook for Now
1) Screen for autobrewery syndrome in patients with episodic fogginess after carb-heavy meals. 2) Run a controlled dietary challenge and serial blood alcohol measurements to confirm. 3) Deploy diet restructuring, antifungals, and probiotics in tandem. 4) Provide patients with documentation and personal testing tools to navigate legal or workplace scrutiny. 5) Follow up with liver panels and symptom logs to refine treatment. This approach turns a diagnostic outlier into a manageable, trackable condition.
The information provided in this article is for general informational purposes only. While we strive for accuracy, we make no guarantees about the completeness or reliability of the content. Always verify important information through official or multiple sources before making decisions.


