Telehealth Abortion Faces a Defining Test
Telehealth Abortion Faces a Defining Test
Telehealth abortion is no longer a niche healthcare workaround – it is quickly becoming one of the clearest fault lines in American medicine. For patients, the stakes are immediate: access, privacy, timing, and cost. For providers, the challenge is even sharper: how do you deliver evidence-based care when state laws, mailing restrictions, and political scrutiny can change faster than clinical guidance? The fight over mifepristone and misoprostol is not just about one treatment pathway. It is about whether remote care can survive as a legitimate, scalable model for reproductive medicine in a fractured legal system. What looks like a dispute over pills is really a stress test for digital healthcare, physician autonomy, and the future of interstate medicine.
- Telehealth abortion has become central to reproductive care access, especially where clinics are scarce or banned.
Mifepristoneandmisoprostolremain at the center of a legal and political fight that goes far beyond medicine.- State-by-state rules are creating a fragmented market where access can depend more on geography than clinical need.
- Providers are balancing patient safety, legal exposure, and logistical complexity in real time.
- The outcome could influence how all forms of telemedicine are regulated across state lines.
Why telehealth abortion matters far beyond abortion care
The immediate issue is straightforward: patients in many parts of the U.S. increasingly rely on remote visits and mailed medication to obtain abortion care. But the larger significance is harder to ignore. Telehealth abortion sits at the intersection of healthcare delivery, digital regulation, pharmacy logistics, and state power. If lawmakers can sharply limit a clinically established telemedicine pathway here, other categories of remote care may eventually face similar pressure.
That is why this issue matters to more than reproductive health advocates. Health systems, digital clinics, compliance teams, and investors in virtual care are all watching the same question: can a doctor licensed and trained to prescribe standard medication still deliver care when politics overrides consistency?
When telemedicine becomes legally unstable in one area of care, every other area starts asking whether it could be next.
For years, telehealth was sold as healthcare’s efficiency upgrade: faster visits, broader reach, lower friction. Reproductive care exposed both the promise and the vulnerability of that model. It works – until geography turns into a legal firewall.
The medication fight is really a system fight
The public conversation often narrows to two drugs: mifepristone and misoprostol. Clinically, they are part of a well-established medication abortion regimen. Politically, they have become symbols in a much bigger struggle over federal authority, state bans, and the power of regulators versus courts.
That matters because healthcare systems depend on predictability. Providers need to know what they can prescribe. Pharmacies need to know what they can dispense. Patients need to know whether a legal treatment available one week will still be available the next. A care model built on uncertainty is hard to scale and harder to trust.
Why mifepristone gets so much attention
Mifepristone has become the focal point because it represents more than a drug. It represents the FDA approval process, the role of evidence in medicine, and the legitimacy of remote prescribing. Challenges to its availability inevitably create ripple effects for telehealth platforms that depend on standardized workflows.
Even when misoprostol-only approaches remain possible in some contexts, the policy pressure around mifepristone sends a broader message: no part of this care pathway is fully insulated from political intervention.
Why mail delivery changes the equation
Mailing medication turns access from a local clinic issue into a logistics issue. That sounds procedural, but it is transformative. Once care can happen by video consult and pharmacy shipment, distance matters less. A patient in a restrictive region may be able to connect with care differently than in the clinic-only era. That is exactly why mailing access has become so contested.
Remote prescribing compresses several barriers at once: travel, scheduling, child care, time off work, and local stigma. It also introduces new stress points: package interception fears, address security, and questions about legal exposure across jurisdictions.
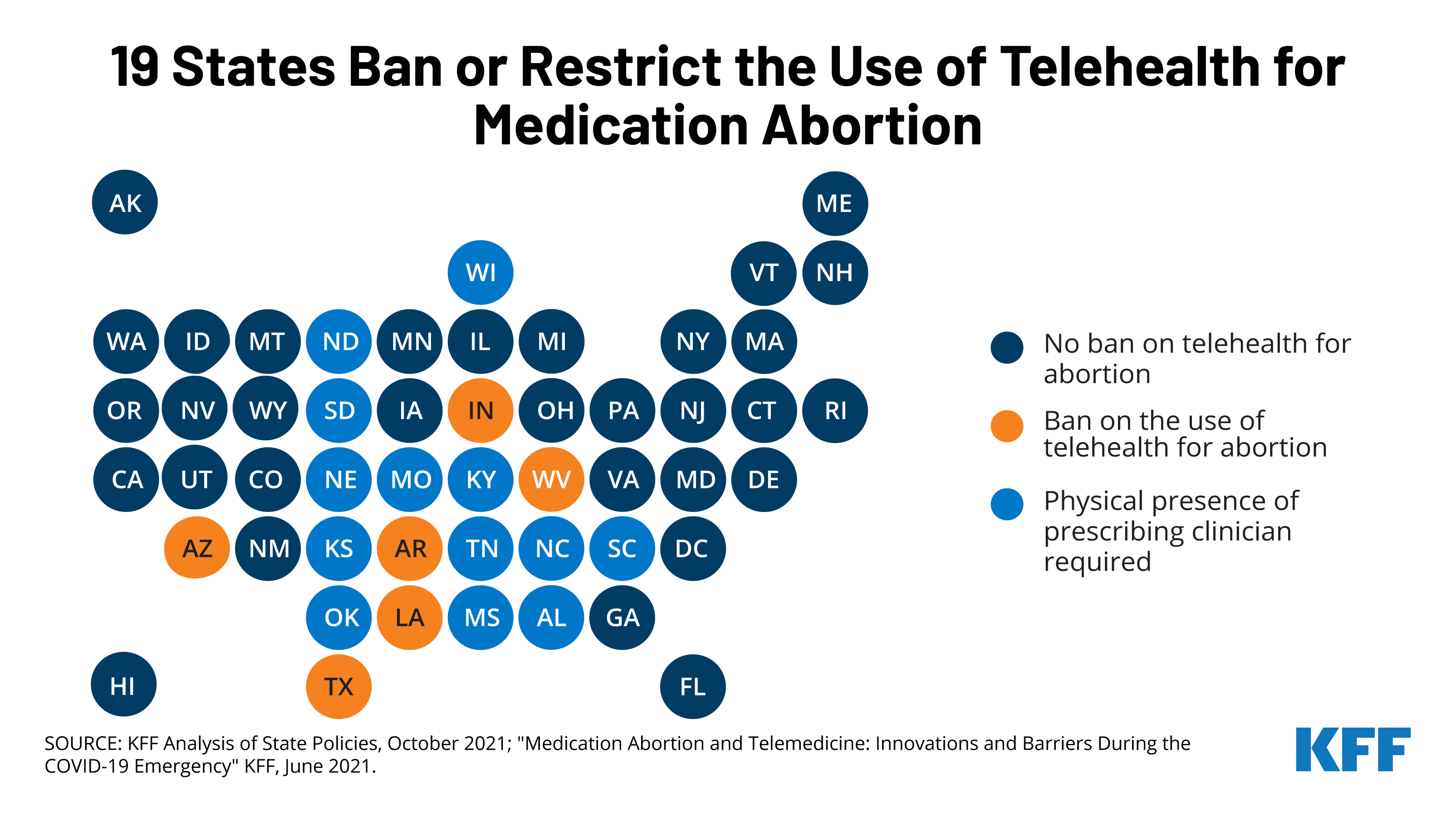
How the state-by-state patchwork is breaking healthcare logic
American healthcare is already fragmented, but telehealth abortion reveals an especially chaotic version of that fragmentation. A patient may have the same medical profile, the same gestational timeline, and the same need for treatment – yet access can change dramatically depending on which side of a state border they are standing on.
From a clinical perspective, that is deeply inefficient. From a patient perspective, it can be devastating. Medication abortion is time-sensitive. Delays are not abstract. A waiting period, a mailing obstacle, or a legal detour can push someone further into pregnancy, force more expensive care, or eliminate options entirely.
- Some states permit telehealth prescribing for abortion medication.
- Some impose restrictions on mailing or clinician presence.
- Some ban abortion care so broadly that telehealth becomes functionally blocked.
- Some create legal ambiguity that chills provider participation even when rules are not fully settled.
This is where the digital health narrative runs into American federalism. Telemedicine wants scale. State regulation imposes borders. The result is a care model that can be technologically modern and legally archaic at the same time.
What providers are actually dealing with
It is easy to frame this as a patient-access story alone, but providers are operating under extraordinary pressure. Physicians and telehealth organizations have to assess not just medical suitability, but licensing, pharmacy coordination, documentation standards, and legal risk. That creates a compliance burden that goes well beyond normal remote care.
Clinical screening is still real medicine
One common misconception is that remote prescribing is casual or thinly supervised. In reality, telehealth abortion protocols typically involve structured intake, medical history review, eligibility assessment, counseling, and follow-up planning. The absence of an in-person visit does not mean the absence of clinical rigor.
Strong programs usually emphasize:
- Clear review of medical history and gestational timing
- Education on expected symptoms and warning signs
- 24/7 or clearly defined follow-up pathways
- Escalation instructions if urgent in-person care is needed
Telemedicine does not remove the need for good medicine. It removes some of the friction around delivering it.
Legal uncertainty can change provider behavior
Even when care is clinically straightforward, legal ambiguity alters behavior. Some clinicians may stop offering services. Some platforms may avoid certain states. Some pharmacies may decline to participate if enforcement risk seems unclear. This is how access contracts before a formal ban even appears: uncertainty does the work of restriction.
That dynamic should concern anyone who cares about healthcare access more broadly. If liability fear can silently narrow legal care, then official policy becomes only part of the story. Market behavior becomes the other half.
Why this is a telemedicine industry story too
The reproductive care debate is also a test case for digital health’s business model. Telemedicine companies are built on the idea that software, clinician networks, and pharmacy partnerships can reduce friction and expand access. That model depends on consistent rules. Once state conflict becomes severe, efficiency gains start to erode.
For the wider industry, there are at least three strategic implications:
- Compliance costs rise: More legal review, state-specific operations, and workflow customization.
- Scaling gets harder: National platforms may have to behave like dozens of mini-regional operators.
- Patient trust becomes fragile: If availability changes unpredictably, consumers may not trust telehealth for high-stakes care.
This is one reason the conflict feels larger than abortion alone. It is a referendum on whether digital healthcare can function as a national infrastructure layer or whether it will remain trapped inside a maze of local exceptions.
What patients need to understand right now
For patients, the biggest challenge is that medically accurate information and legally actionable information are no longer always the same thing. A person may be clinically eligible for medication abortion and still face barriers tied to residence, mailing address, or provider availability.
That makes clarity essential. Patients navigating this space often need to verify:
- Whether telehealth abortion is permitted where they are located
- Whether a provider can legally prescribe across that jurisdiction
- What follow-up support exists if complications or questions arise
- How quickly medication can realistically arrive
Pro Tip: Time sensitivity matters. In any care pathway where timing can affect options, delays caused by uncertainty are not minor administrative problems – they can materially change outcomes.
The future of telehealth abortion could reshape remote care policy
If there is one reason this story deserves close attention, it is this: the legal treatment of telehealth abortion may set the tone for how states approach remote medicine more broadly. Once policymakers establish that certain categories of approved medication can be singled out, routed through special restrictions, or blocked across borders, the precedent becomes difficult to contain.
The interstate medicine question is only getting bigger
Telehealth has always challenged an old assumption: that care is inherently local. Patients now expect clinicians to be digitally reachable. Providers expect software to bridge distance. Regulators, however, still often think in state lines. That mismatch is becoming impossible to ignore.
Expect future debates to focus on:
- Cross-state licensure and enforcement
- Mail-order pharmacy authority
- Digital platform responsibility for restricted care categories
- Data privacy for sensitive health interactions
Policy volatility is now part of care design
One of the less discussed consequences of this fight is that care design itself is changing. Telehealth providers can no longer think only like medical organizations. They also have to think like risk managers, logistics coordinators, and policy analysts. Workflows increasingly need contingency planning built in.
In practical terms, that means operations may begin to look more like this:
intake -> eligibility review -> jurisdiction check -> pharmacy pathway -> shipment timing -> follow-up support
That sequence is not just about medicine. It is about surviving legal complexity without compromising patient care.
The bottom line
The battle over mifepristone, misoprostol, and mail-based access is not a narrow healthcare dispute. It is a defining conflict over whether modern medicine can be delivered through modern channels when politics disapproves of the outcome. Patients see the human cost first: delays, uncertainty, lost access. Providers see the operational burden next: fragmented rules, legal ambiguity, and shrinking room to practice evidence-based care.
But the larger lesson is harder to miss. Telehealth promised to make care less dependent on location. Reproductive medicine is showing exactly how fragile that promise becomes when law, not science, dictates the boundaries of treatment. If telehealth abortion can be constrained despite established clinical use and clear patient demand, then the future of remote care in America looks less like seamless innovation and more like a map of exceptions.
That is why this moment matters: not only for abortion access, but for the credibility of telemedicine itself.
The information provided in this article is for general informational purposes only. While we strive for accuracy, we make no guarantees about the completeness or reliability of the content. Always verify important information through official or multiple sources before making decisions.